
Functional Medicine for
Eosinophilic Esophagitis (EoE)
You've been told your esophagus is inflamed. You've been given reflux medication that doesn't fully work. You've watched your food list shrink and your anxiety around meals grow. There is another way to look at this.
1 in 700
Americans Affected By
EOE
5x
Increase in Prevalence
since 2009
$1.3B
Annual U.S. Healthcare
costs
75%
of EOE patients have co-occurring atopic disease
Understanding your Diagnosis
Why Eosinophilic Esophagitis (EoE) is More Than Just an Allergic Condition
If you've been recently diagnosed with EoE — or have been struggling for years without answers — you're not alone. And you deserve more than a prescription that doesn't address why your immune system is attacking your own esophagus.
Imagine sitting down to a meal and feeling food stop somewhere between your throat and your stomach. Or eating your favorite dish and ending up in the emergency room because something got lodged. Maybe it's the persistent heartburn that no antacid or acid blocker has touched for years. These experiences are real, exhausting, and disruptive to daily life — and they are the hallmark of a condition called Eosinophilic Esophagitis, or EoE.
EoE is a chronic, immune-mediated inflammatory disease of the esophagus — the muscular tube that carries food and liquid from your mouth to your stomach. In people with EoE, a type of white blood cell called an eosinophil, which normally has no place in a healthy esophagus, accumulates in the esophageal lining in large numbers. This build-up causes persistent inflammation, and over time, can lead to scarring, narrowing, and structural changes that make swallowing increasingly difficult and dangerous.
Here is what the conventional medical system often fails to address: EoE is not just an allergy. It is a systemic immune dysfunction rooted in the gut, the microbiome, environmental exposures, and a breakdown of the body's barrier systems. Functional medicine asks the deeper question — not just "what is the diagnosis?" but "why is the immune system behaving this way, and what can we do to change the conditions that are driving it?"

A key insight: Research published in Clinical Gastroenterology and Hepatology (2025) reports that EoE prevalence has increased five-fold since 2009, affecting approximately 1 in 700 Americans — with over 472,000 estimated cases in the United States alone. Annual healthcare costs associated with EoE now exceed $1.3 billion. This is not a rare or trivial condition. (Source: Thel et al., Clin Gastroenterol Hepatol. 2025;23:272–280)

The Science of EoE
What Is Eosinophilic Esophagitis? A Deeper Look
Understanding what is actually happening in the body is the first step toward meaningful healing.
In a healthy esophagus, eosinophils are absent. Their presence — particularly when they exceed 15 per high-power field on biopsy — is the diagnostic cornerstone of EoE. But why do they show up there in the first place?
EoE is driven by a Type 2 T-helper cell (Th2) immune response — the same branch of the immune system responsible for allergic conditions like asthma, eczema, and hay fever. When the immune system encounters food or environmental antigens (such as proteins from dairy, wheat, eggs, soy, or airborne pollens), it can trigger an inflammatory cascade in the esophageal tissue. Cytokines like interleukin-4, interleukin-5, and interleukin-13 are released, recruiting eosinophils and mast cells to the esophagus, causing the characteristic inflammation and tissue damage.
Unlike classic IgE-mediated food allergies that cause immediate reactions (hives, throat swelling), EoE typically involves a delayed hypersensitivity response — which is one reason it's so difficult to pinpoint. A food eaten days earlier could be the culprit for today's symptoms.
The Role of Esophageal and Gut Microbiome
Emerging research published in Scientific Reports (Nature) has confirmed that patients with active EoE show measurable changes in both their esophageal and intestinal microbiome compared to healthy individuals. Imbalances in species such as Fusobacterium, Lactobacillus, Bifidobacterium, and Veillonella have been observed in people with EoE. (Source: PLOS One, Esophageal Microbiome in EoE; Scientific Reports 2021)
Dysbiosis — or an imbalance in the microbial community — may trigger inappropriate immune responses and promote eosinophilic accumulation in the esophageal tissue. This is not just a theory; it is an active area of research with growing clinical implications for how we approach the condition.
Intestinal Permeability and the "Leaky Gut" Connection
A compromised gut lining — commonly referred to as increased intestinal permeability or "leaky gut" — allows food proteins and inflammatory compounds to pass into the bloodstream more easily, triggering heightened immune reactions. Research supports the esophageal epithelium itself as an area of disturbed permeability in EoE, with the barrier function of the esophageal lining playing a central role in how antigens are recognized and how the Th2 allergic pathway is initiated.
Important finding: Early-life factors — including cesarean birth, formula feeding, and antibiotic exposure in infancy — have been linked to increased EoE risk. These are all known to disrupt the healthy development of the infant microbiome, reinforcing the idea that gut health and immune programming are inseparably linked. (Source: PMC, Epidemiology of EoE, 2025)
Genetic and Environmental Factors
EoE has a meaningful genetic component — with 31 genes potentially associated with increased susceptibility, and a 7% rate of positive family history among those diagnosed. However, twin studies confirm that genetics alone cannot explain the disease. Environmental and epigenetic factors play an equally important role, which is why EoE rates are rising primarily in industrialized, high-income countries — and why a whole-person approach to care matters so much.
Recognizing EOE
Symptoms of Eosinophilic Esophagitis Across All Ages
EoE presents differently depending on age. Symptoms in children often mimic colic or GERD, while adults more commonly experience dysphagia and food impaction.
One of the most frustrating aspects of EoE is how long it can take to receive a proper diagnosis. Symptoms can be present for years before EoE is correctly identified — often because they overlap with many other conditions, and because many practitioners are still unfamiliar with the disease.
Symptoms vary by age and severity:
Adults: Difficulty swallowing (dysphagia), food impaction (food getting stuck—sometimes a medical emergency), chest pain, regurgitation, or heartburn that doesn’t respond well to antacids.
Children: Feeding refusal, vomiting, abdominal pain, poor growth (failure to thrive), or recurrent reflux-like symptoms.
Many describe “silent” progression until scarring occurs. Over time, ongoing inflammation can lead to narrowing of the esophagus (strictures), making symptoms progressively worse if not addressed. If you’ve been told your reflux or swallowing issues are “just GERD” but nothing helps, EoE may be worth exploring.

Seasonal variability is real: Because aeroallergens (pollen, mold, dust mites) can trigger EoE flares, many patients notice their symptoms worsen in spring and summer. EoE is in fact diagnosed more commonly during high-pollen seasons, which underscores the environmental — not purely dietary — nature of the disease.
Getting Answers
How EoE Is Diagnosed — And Why It's Often Missed
Diagnosis requires more than symptoms. It requires endoscopic biopsy — and careful exclusion of conditions that look just like EoE.
Diagnosis typically involves an upper endoscopy (EGD) with multiple biopsies from different esophageal levels. Doctors use scoring systems like the EoE Endoscopic Reference Score (EREFS) to assess rings, furrows, exudates, edema, and strictures. Allergy testing alone doesn’t diagnose EoE, but it can help identify potential triggers.
Conditions That Can Mimic EoE
Before confirming an EoE diagnosis, several other conditions must be carefully ruled out — some of which require entirely different management strategies.
This is one of the most important and under-discussed aspects of EoE care. The symptoms of EoE — dysphagia, heartburn, chest pain, regurgitation — are shared by many other conditions. Even the finding of elevated eosinophils on biopsy alone is not sufficient to diagnose EoE; other diseases can also cause esophageal eosinophilia.
CONDITION
GERD (Gastroesophageal Reflux Disease)
Achalasia
Hypereosinophilic Syndrome (HES)
Celiac Disease
Crohn’s Disease
Eosinophilic Gastroentieritis
Infectious Esophagitis
Pill Esophagitis (Drug-Induced)
HOW IT MIMICS EOE
Heartburn, regurgitation, chest pain, even mild esophageal eosinophilia on biopsy
Dysphagia to both solids and liquids, regurgitation, chest pain
Elevated eosinophils in esophageal tissue
KEY DISTINGUISHING FEATURES
GERD typically responds to PPIs; eosinophilia concentrated in distal esophagus only; erosive esophagitis more common
Caused by failure of the lower esophageal sphincter to relax; diagnosed with esophageal manometry; no eosinophilia on biopsy
HES causes eosinophilia throughout multiple organ systems (heart, lungs, skin, GI tract), not limited to the esophagus; elevated peripheral blood eosinophil count
GI symptoms, food reactions, nutritional deficiencies, immune dysregulation
Celiac is triggered specifically by gluten; diagnosed via serologic testing (tTG-IgA) and small bowel biopsy; villous atrophy is characteristic
Esophageal involvement causing dysphagia and inflammation; esophageal eosinophilia
Crohn's typically causes inflammation throughout the entire GI tract; granulomas on biopsy; abnormal colonoscopy findings
Eosinophilic inflammation causing GI symptoms including dysphagia
Affects stomach and small intestine in addition to esophagus; eosinophilia present outside the esophagus on biopsy
Odynophagia (painful swallowing), dysphagia, chest discomfort
Usually caused by Candida (fungal), HSV, or CMV; more common in immunocompromised individuals; specific histologic findings on biopsy
Chest pain, dysphagia, odynophagia after medication use; esophageal eosinophilia
Caused by direct mucosal injury from medications (antibiotics, NSAIDs, bisphosphonates); history of recent new medication is key
Mast Cell Activation Syndrome (MCAS)
Multi-system allergic symptoms including GI inflammation, food reactions, esophageal involvement
MCAS involves dysregulated mast cell activation across multiple organ systems; responds to antihistamines and mast cell stabilizers
Connective Tissue Disorders
Esophageal dysmotility and inflammation (e.g., in scleroderma, Marfan syndrome, hypermobile EDS)
Systemic findings such as skin, joint, or vascular involvement; specific antibody panels and genetic testing
Why Functional Medicine Testing Adds Valuable Context
Because these conditions so frequently overlap or coexist with EoE, a thorough functional medicine evaluation that goes beyond a single biopsy finding is essential. Many EoE patients also carry comorbid diagnoses of GERD, asthma, eczema, seasonal allergies, and even autoimmune thyroid disease — all of which share underlying roots in immune dysregulation. While endoscopy remains essential, functional medicine offers additional investigative tools that conventional GI workups do not include. These can help uncover contributing drivers and guide a personalized healing plan:
Comprehensive stool analysis with microbiome profiling
SIBO (Small Intestinal Bacterial Overgrowth) breath testing
Intestinal permeability / leaky gut assessment
Histamine intolerance markers (DAO enzyme levels)
Environmental allergy panel (aeroallergens, mold, dust mites)
Nutritional status assessment (deficiencies common from restricted diets)
Comprehensive food sensitivity panels (IgG and IgA-mediated delayed reactions)
H.pylori stool antigen testing
Fecal eosinophil protein X (EPX) - a marker of eosinophilic activity
Mast Cell Activation Syndrome (MCAS) evaluation
Genetic SNP testing (e.g., MTHFR, CAPN14 variants)
Inflammatory markers (CRP, IL-5, IgE levels)
Rather than managing symptoms indefinitely, functional medicine works to identify and address the upstream factors that are driving the immune dysfunction in the first place.
Conventional management of EoE typically focuses on three pillars: dietary restriction, swallowed topical corticosteroids (like budesonide or fluticasone), and proton pump inhibitors. While these approaches can reduce inflammation and provide relief, they do not address the underlying reasons the immune system became dysregulated. Long-term steroid use carries risks including Candida overgrowth and adrenal suppression, and symptom return is common once interventions are stopped.
Functional medicine does not replace gastroenterology care — endoscopy and biopsy monitoring remain essential for anyone with EoE. What functional medicine adds is a systematic investigation into the environmental, dietary, microbial, and genetic factors that are sustaining the inflammatory state — and personalized strategies to shift the body's terrain.
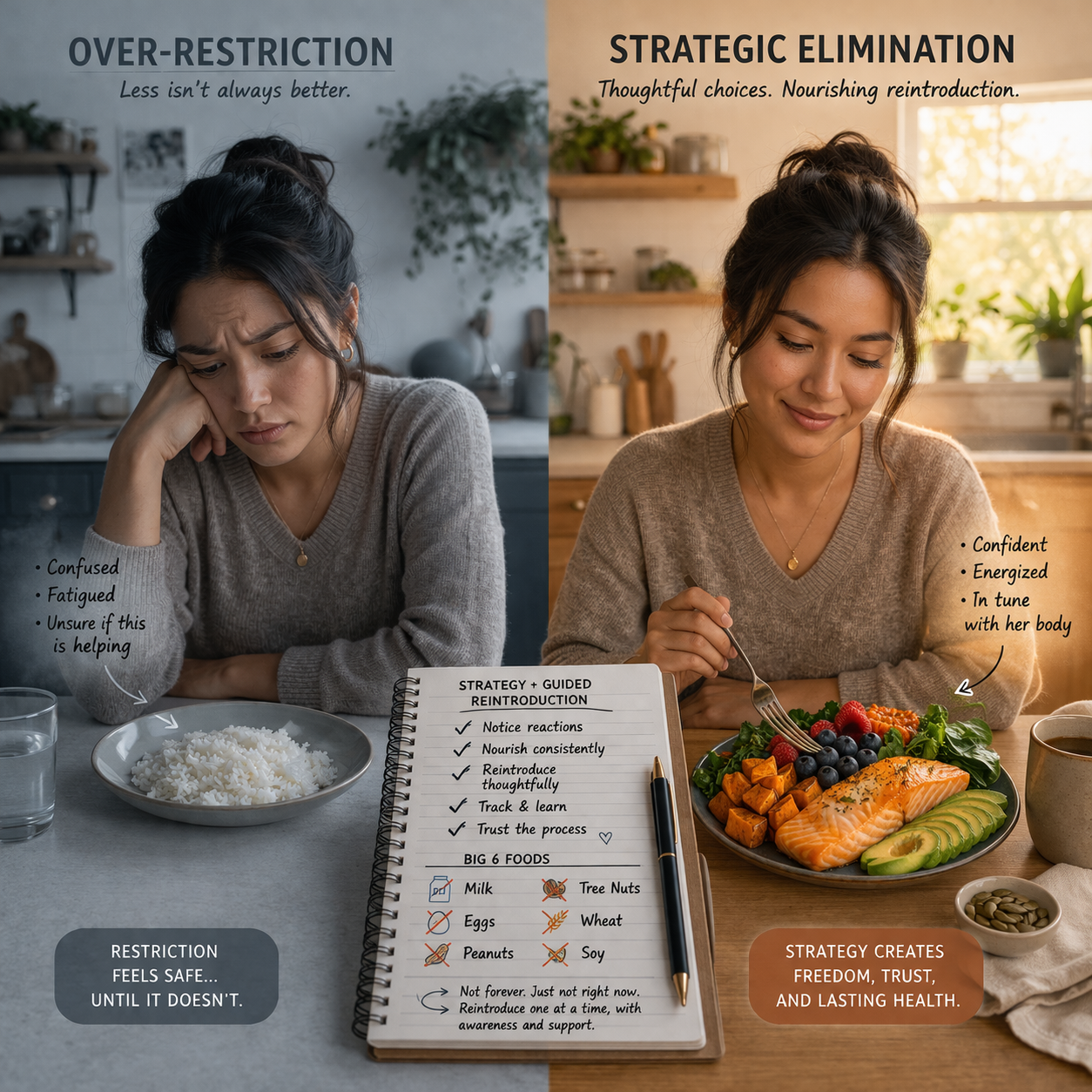
Identify and Remove Dietary Triggers Foods are a primary trigger for most people with EoE. Many find significant relief through structured elimination diets (such as the six-food elimination diet removing dairy, wheat, eggs, soy, nuts, and seafood). We guide you step-by-step with reintroduction protocols and follow-up testing to identify your unique triggers—often more comprehensive than standard allergy panels.
Restore Gut Microbiome Balance Research confirms altered microbial populations in both the esophageal and intestinal microbiome in EoE patients. Targeted probiotic and prebiotic protocols — particularly those incorporating Bifidobacterium and Lactobacillus species — may help modulate the immune response, reduce inflammation, and restore barrier integrity. Synbiotic mixtures have shown promise in improving symptoms such as chest pain and appetite in EoE patients.
Heal Intestinal Permeability A compromised gut lining allows food proteins and pro-inflammatory molecules to access the bloodstream, amplifying the immune response throughout the body — including in the esophagus. Gut-healing protocols may include targeted nutrients such as L-glutamine, zinc carnosine, collagen, deglycyrrhizinated licorice (DGL), and anti-inflammatory botanical compounds to restore mucosal integrity.
Holistic lifestyle factors Stress, sleep, environmental exposures, and seasonal allergens can all influence Th2-driven responses. We incorporate mind-body practices, optimized hydration, mindful eating habits, and natural anti-inflammatory approaches (omega-3-rich foods, quercetin-rich plants) to promote overall resilience.
Support Nutritional Repletion Extended elimination diets and chronic inflammation create significant risks for nutritional deficiencies — including deficiencies in calcium, vitamin D, B12, iron, and zinc. Functional medicine ensures that dietary restriction does not come at the cost of nutritional adequacy, using targeted supplementation and nutrient-dense whole food protocols tailored to each patient's tested needs.
Reduce the Total Inflammatory Burden Chronic stress, poor sleep, sedentary lifestyle, and processed food consumption all amplify systemic inflammation and immune dysregulation. Functional medicine addresses these lifestyle drivers holistically — because healing the esophagus requires calming the entire immune system, not just the tissue in question. Mind-body practices, sleep hygiene optimization, and anti-inflammatory lifestyle strategies are integral parts of care.
Comprehensive testing and monitoring We may assess food sensitivities, microbiome health, nutrient levels, or inflammatory markers to create a truly individualized plan. This root-cause lens helps many people feel more in control while working alongside their gastroenterologist.
Functional medicine does not replace conventional care (such as PPIs, topical steroids, biologics like dupilumab, or dilation when needed). Instead, it complements it by addressing the “why” behind the immune overreaction and supporting long-term esophageal and whole-body wellness.
DIET & NUTRITION
The Six-Food Elimination Diet and Beyond
Diet is one of the most powerful levers in EoE care — but elimination without strategy can leave you nutritionally depleted and still symptomatic.
The six-food elimination diet (SFED), originally developed and studied by Kagalwalla et al. (2006), removes the most common dietary triggers of EoE. Clinical evidence demonstrates that this approach leads to histologic improvement in a significant proportion of patients, with some achieving complete mucosal healing. Foods are eliminated for a period of 6–8 weeks, followed by structured reintroduction with repeat endoscopy to identify specific triggers.
Common EoE dietary triggers (the “Big 6”): Dairy/Cow’s Milk, Wheat/Gluten, Eggs, Soy, Tree Nuts & Peanuts, Seafood/Shellfish
Beyond the Big 6, functional medicine also evaluates for individual food sensitivities through IgG and IgA antibody testing, reactions to high-histamine foods (fermented foods, aged cheeses, alcohol, cured meats), and cross-reactivity between food proteins and environmental allergens (oral allergy syndrome).
Healing and anti-inflammatory foods to emphasize: wild-caught salmon, leafy greens, berries, sweet potato, turmeric & ginger, bone broth, olive oil, coconut products, zucchini, avocado, pumpkin seeds, chamomile tea
Mindful Eating and the Mealtime Environment
How you eat matters as much as what you eat. Eating slowly, chewing food thoroughly (a minimum of 20–30 chews per bite), remaining upright for 30–45 minutes after meals, and eating in a calm, unstressed state all reduce the mechanical and inflammatory burden on the esophagus. Many EoE patients develop significant anxiety around meals — addressing this with a functional medicine team, and potentially with a therapist familiar with chronic illness, is an important part of whole-person care.
Your Questions, Answered
-
No. EoE involves a delayed, non-IgE-mediated hypersensitivity response — meaning the immune reaction is slower and not the same mechanism as classic IgE-mediated anaphylactic food allergies (like a peanut allergy that causes immediate hives or throat swelling). This is why standard allergy skin-prick tests often don't accurately identify EoE food triggers, and why specialized food sensitivity panels used in functional medicine are often more informative.
-
Some patients do follow a "waxing and waning" course with periods of reduced symptoms, and rare cases of apparent spontaneous remission have been reported. However, symptom improvement does not equal tissue healing — it is entirely possible to feel better while ongoing eosinophilic inflammation continues to damage the esophageal tissue. This is why endoscopic monitoring remains essential even during asymptomatic periods. Functional medicine works to support the conditions for sustained remission, but cannot guarantee it, and should always be pursued alongside appropriate medical monitoring.
-
GERD is caused by acid from the stomach flowing backward into the esophagus, causing localized mucosal injury. It typically responds to acid-suppressing medications. EoE is an immune-mediated condition driven by food and environmental allergens that does not respond to acid suppression. On endoscopy, GERD tends to cause erosive changes and ulceration in the distal esophagus, while EoE causes rings, furrows, white exudates, and edema throughout the entire esophagus. Importantly, the two conditions frequently coexist, and up to half of EoE patients also have GERD.
-
The six-food elimination diet (SFED) removes the six most common EoE triggers — dairy, wheat, eggs, soy, tree nuts/peanuts, and seafood/shellfish — for 6–8 weeks. A repeat endoscopy is then performed to evaluate tissue-level improvement. Foods are then reintroduced one at a time, with endoscopy after each reintroduction, to identify which specific foods are driving inflammation in that individual. This structured approach identifies personal triggers more precisely than empirical broad restriction.
-
Yes. Chronic psychological stress activates immune and inflammatory pathways — including mast cell degranulation and increases in gut permeability — that can amplify EoE symptoms and flares. Stress does not cause EoE on its own, but it can meaningfully worsen the inflammatory burden. Mind-body practices including meditation, breathwork, and yoga are not optional extras in holistic EoE care — they are biologically relevant interventions that address the stress-immune connection directly.
-
EoE is considered a chronic condition, and current evidence does not support the idea that children reliably outgrow it in the way they might outgrow some food allergies. Some children may experience periods of reduced symptoms, particularly with dietary management, but ongoing monitoring is recommended. The structural changes that can develop with untreated inflammation — including scarring and strictures — underscore the importance of consistent care, not a "wait and see" approach.
-
A functional medicine approach focuses on identifying underlying contributors such as food sensitivities, gut health imbalances, inflammation, and environmental triggers. The goal is to support the body’s systems and reduce immune reactivity through a personalized strategy.
-
EOE is not classified as a traditional autoimmune disease, but it is an immune-mediated condition. It involves an overactive immune response, often linked to allergic and inflammatory pathways.
-
Yes, EOE is commonly associated with:
Asthma
Eczema
Seasonal allergies
Other digestive conditions
This connection highlights the role of the immune system in the condition.
Ready to Explore the Root Cause of Your EoE?
Our functional medicine approach combines the latest science with individualized care — so you can do more than just manage EoE, you can work toward lasting healing.