
Functional Medicine for POTS (Postural Orthostatic Tachycardia Syndrome)
A Whole-Body Approach to POTS and Autonomic Nervous System Dysfunction

POTS — Postural Orthostatic Tachycardia Syndrome
Symptoms, Causes & Root-Cause Treatment: The Underlying Imbalances That Drive POTS
You stand up and your heart races. The room spins. You feel like you might faint. Brain fog settles in so thick you can barely form a sentence. And when you finally see a doctor, the tests come back inconclusive — or you're handed a beta blocker and told to drink more water. If this sounds familiar, you are not alone — and you are not imagining it.
POTS is a form of dysautonomia — a dysfunction of the autonomic nervous system — that affects an estimated 1 to 3 million Americans, the majority of whom are women between the ages of 15 and 50. It is significantly underdiagnosed, frequently misunderstood, and often dismissed entirely. At Premier IFM in Placentia, Orange County, we take POTS seriously — and more importantly, we look for why it developed in the first place.
POTS is not a diagnosis you manage with salt tablets and compression socks and accept as a life sentence. It is a signal — and like every signal the body sends, it has a cause worth finding.
You are not alone!
POTS affects far more people than most doctors realize — and the majority of them looked completely normal on the outside while quietly struggling through every day. The numbers below begin to tell a story that has been largely overlooked by conventional medicine for far too long.
Americans estimated to have POTS — many undiagnosed
Of POTS patients are women, primarily ages 15–50
~6 yrs
Average time to diagnosis — often after multiple misdiagnoses
Beats per min. heart rate increase upon standing required for diagnosis
77% - Of POTS patients were told their symptoms were psychiatric or psychological before receiving their correct diagnosis.
The same large-scale survey found that patients see an average of 7 different doctors before receiving a correct POTS diagnosis — and 15% of patients wait over 10 years before anyone connects the dots.
What is POTS?
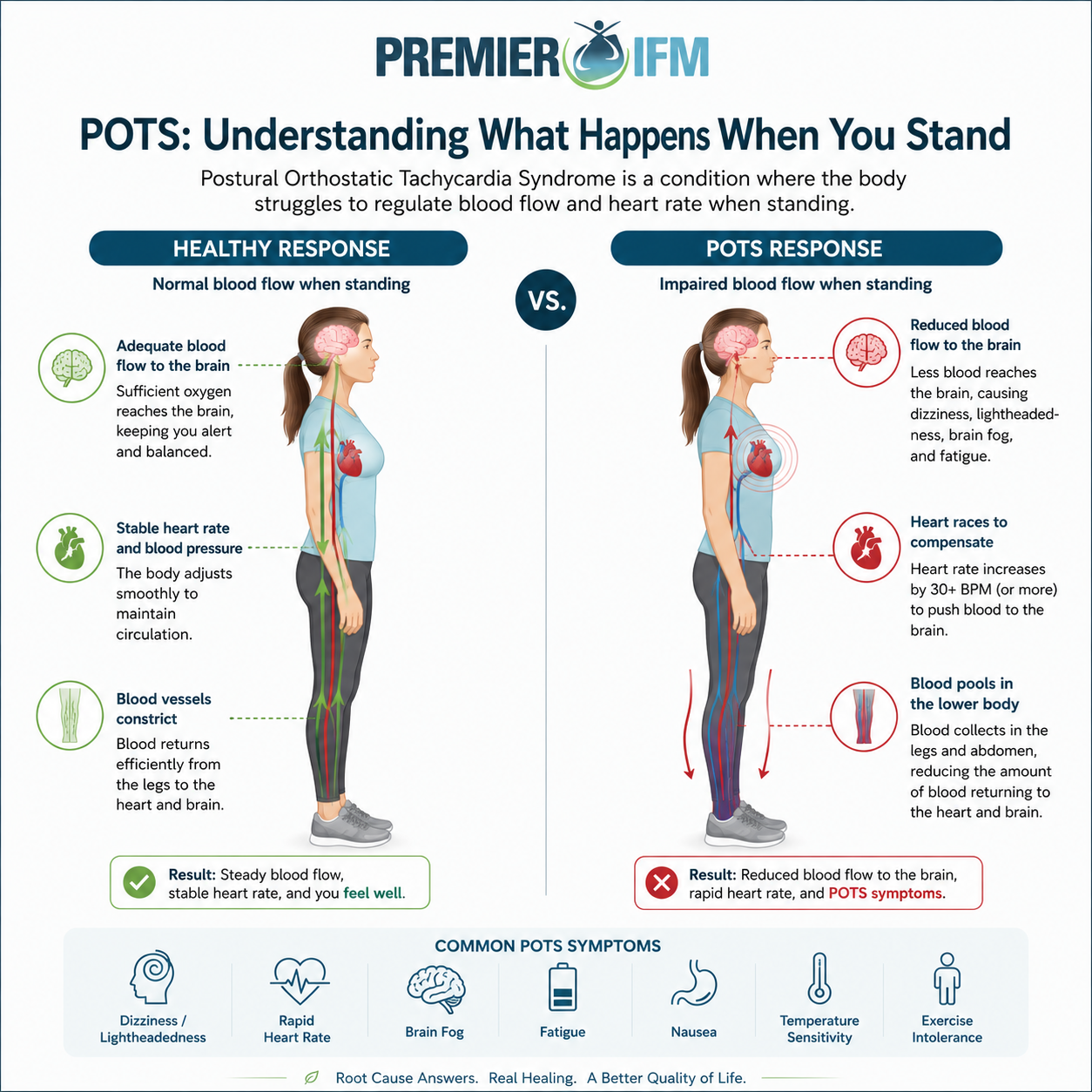
POTS stands for Postural Orthostatic Tachycardia Syndrome. It is a condition in which the autonomic nervous system — the part of the nervous system that controls automatic functions like heart rate, blood pressure, digestion, and circulation — fails to properly regulate the cardiovascular response when a person moves from lying down or sitting to standing upright.
In a healthy individual, the body automatically adjusts blood flow when you stand — constricting blood vessels in the lower extremities to maintain adequate circulation to the brain and vital organs. In POTS, this mechanism fails. Blood pools in the legs and lower body, the brain receives insufficient blood flow, and the heart compensates by beating excessively fast — typically 30 or more beats per minute faster than when lying down.
The result is a cascade of symptoms that can range from mildly disruptive to completely disabling — and because the symptoms overlap with anxiety, chronic fatigue, and other common conditions, POTS is notoriously difficult to diagnose in conventional medical settings.
Formally defined: POTS is diagnosed when a patient experiences a sustained heart rate increase of 30 or more beats per minute (40+ in adolescents) within 10 minutes of standing, in the absence of orthostatic hypotension, accompanied by symptoms of orthostatic intolerance. - Heart Rhythm Society Consensus Statement
Symptoms of POTS
POTS symptoms are wide-ranging because the autonomic nervous system regulates so many body functions simultaneously. This is one reason it takes so long to diagnose — symptoms often appear unrelated.
💓 Heart racing upon standing -Rapid heart rate increase of 30+ BPM when moving to upright position
😵 Lightheadedness & dizziness - Feeling faint, unsteady, or like the room is spinning — especially when standing
🧠 Brain fog - Cognitive difficulty, difficulty concentrating, memory problems, mental fatigue
😴 Extreme fatigue - Debilitating exhaustion disproportionate to activity level — often worse after standing
👁️ Visual disturbances - Tunnel vision, blurred vision, or darkening of vision when standing or during exertion
🤢 Nausea - Gastrointestinal symptoms including nausea, bloating, and altered motility
🌡️ Temperature dysregulation - Inability to tolerate heat, excessive sweating or lack of sweating, cold extremities
😰 Anxiety-like symptoms - Trembling, shakiness, chest tightness — often misdiagnosed as anxiety disorder
😴 Sleep disturbances - Non-restorative sleep, insomnia, waking unrefreshed regardless of sleep duration
💪 Exercise intolerance -Severe worsening of symptoms with even mild physical activity — post-exertional malaise
🩸 Blood pooling - Visible discoloration or mottling of legs and feet when standing; dependent acrocyanosis
🤯 Headaches - Chronic headaches and migraines, often positional and worsened by standing or activity
⚠Important: Because these symptoms overlap with anxiety, panic disorder, chronic fatigue syndrome, and other conditions, many POTS patients spend years — sometimes over a decade — being misdiagnosed or dismissed before receiving an accurate diagnosis.
Types of POTS
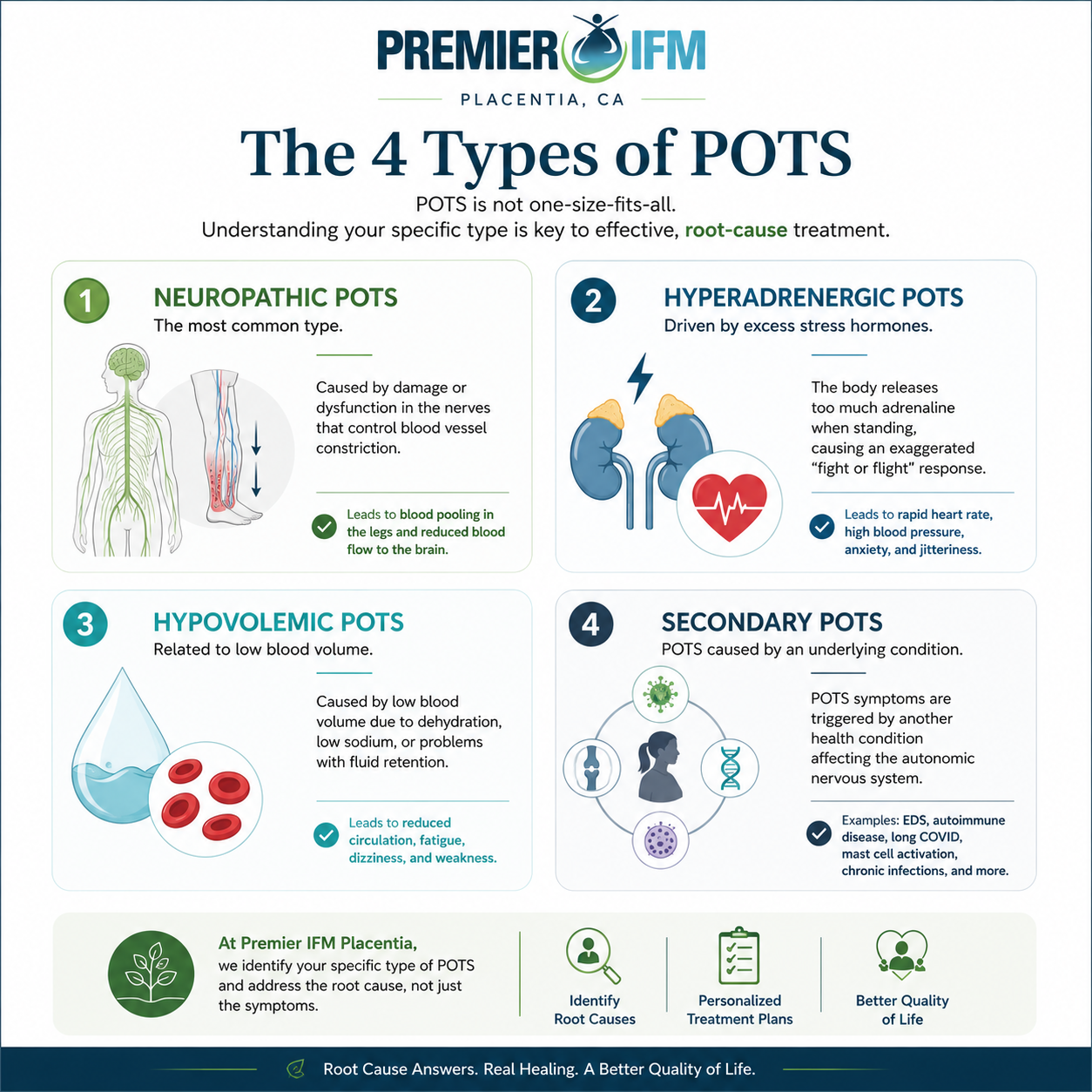
POTS is not a single condition — it is a syndrome with several distinct subtypes, each with different underlying mechanisms. Identifying which type a patient has is critical to finding the right approach.
Neuropathic POTS: The most common subtype. Caused by partial peripheral autonomic neuropathy — small nerve fibers in the lower body fail to adequately constrict blood vessels upon standing, causing blood pooling.
Hyperadrenergic POTS: Characterized by elevated norepinephrine levels. The nervous system overproduces stress hormones in response to standing, resulting in extreme symptoms including high blood pressure, tremors, and anxiety.
Hypovolemic POTS: Driven by low blood volume. The body simply does not have enough circulating blood to maintain adequate perfusion when standing. Often linked to hormonal dysregulation including aldosterone and renin imbalance.
Secondary POTS: Develops as a consequence of another underlying condition — autoimmune disease, Ehlers-Danlos syndrome (EDS), diabetes, mast cell activation syndrome (MCAS), Lyme disease, or post-viral illness including long COVID.
What Most People Don't Know About POTS
Here is where the research gets genuinely interesting — and where conventional medicine often falls short of the full picture.
POTS dramatically increased after COVID-19. Post-COVID POTS has become one of the most significant emerging autonomic disorders. Studies estimate that POTS symptoms develop in a meaningful percentage of long COVID patients, making it one of the most prevalent post-viral autonomic syndromes ever documented.
POTS is frequently associated with autoimmune activity. Research has identified autoantibodies — immune proteins that attack the body's own tissues — targeting adrenergic and muscarinic receptors in the autonomic nervous system in a significant subset of POTS patients. This suggests that for many patients, POTS may have an autoimmune component.
Up to 50% of POTS patients also have Mast Cell Activation Syndrome (MCAS). The overlap between POTS and MCAS is striking and clinically significant. Mast cells release histamine and other mediators that cause blood vessel dilation and worsen orthostatic intolerance. This overlap is frequently missed in conventional workups.
POTS and Ehlers-Danlos Syndrome (EDS) commonly co-occur. The hypermobile form of EDS — a connective tissue disorder that can contribute to excessive venous pooling and impaired blood vessel support, worsening orthostatic intolerance. — is found at disproportionately high rates in POTS patients. Connective tissue laxity allows excessive venous pooling and contributes directly to orthostatic intolerance.
Small fiber neuropathy is present in a significant percentage of POTS patients. Research has identified reduced small nerve fiber density in a subset of POTS patients using skin punch biopsy testing, supporting the presence of structural autonomic nerve abnormalities in some cases of POTS, not just nervous system dysregulation.
Gut dysfunction is common in POTS and may be both a cause and consequence. Gut dysfunction is increasingly recognized in POTS and dysautonomia. The enteric nervous system — often called the body’s ‘second brain’ — is closely connected to autonomic regulation. Research has identified altered gut microbiota, gastrointestinal symptoms, and motility disturbances in many POTS patients, suggesting that gut dysfunction may contribute to autonomic imbalance through inflammatory, neurological, and immune pathways.
Many POTS patients have low blood volume — but not for the reason you'd expect. Research has found that POTS patients often have reduced plasma volume not simply from dehydration, but from hormonal dysregulation affecting aldosterone, renin, and erythropoietin — the hormones that control blood volume. Simply drinking more water doesn't fix a hormonal dysregulation.
Common Root Causes & Contributing Factors in POTS
One of the biggest misconceptions about POTS is that it is simply a “heart rate problem.”
In reality, POTS is often a complex, multi-system condition involving the nervous system, circulation, immune system, hormones, inflammation, and gut health. This is why two people with POTS can experience very different symptoms—and why a one-size-fits-all treatment approach often falls short.
At Premier Integrative & Functional Medicine, we focus on identifying the underlying imbalances contributing to autonomic dysfunction so we can better support long-term healing and stability.
Nervous System Dysregulation
POTS is fundamentally a disorder of the autonomic nervous system—the system responsible for controlling automatic functions like heart rate, blood pressure, circulation, digestion, and temperature regulation.
In many patients, the nervous system becomes stuck in a chronic “fight-or-flight” state, causing:
excessive adrenaline release
rapid heart rate
dizziness
anxiety-like symptoms
exercise intolerance
Rather than properly adapting to stress and posture changes, the body remains in a constant state of overactivation and compensation.
Gut Dysfunction & the Gut-Brain Connection
The gut and nervous system are deeply connected through the gut-brain axis and enteric nervous system — often called the body's 'second brain.' Gut dysbiosis, intestinal permeability, and SIBO generate systemic inflammation that can directly disrupt autonomic regulation and contribute to blood volume abnormalities. What makes this connection particularly important in POTS is that it works in both directions — gut dysfunction can drive autonomic dysregulation, and autonomic dysfunction can worsen gut motility and barrier integrity, creating a cycle that is difficult to break without addressing both systems simultaneously.
Autoimmune Activity & Immune Dysregulation
Studies have identified autoantibodies targeting adrenergic and muscarinic receptors involved in autonomic nervous system regulation. In other words, the immune system may mistakenly interfere with the body’s ability to regulate circulation and heart rate properly.
Many patients also report the onset of POTS symptoms after:
viral illness
COVID-19
infection
major stressors
surgery
This suggests that immune activation may play an important role in triggering or worsening symptoms.
Nutrient Deficiencies & Mitochondrial Stress
Low levels of nutrients such as:
iron
B12
B1 (thiamine)
magnesium
electrolytes
Vitamin D
can impair nervous system function, circulation, oxygen delivery, and energy production.
Many POTS patients also experience mitochondrial dysfunction and reduced cellular energy production, contributing to severe fatigue and exercise intolerance.
Small Fiber Neuropathy
Some POTS patients have evidence of small fiber neuropathy—a condition involving damage to small autonomic nerve fibers.
These nerves help regulate:
blood vessel constriction
circulation
sweating
heart rate responses
When damaged, the body may lose its ability to properly control blood flow and autonomic function.
Studies using skin punch biopsies have identified reduced small nerve fiber density in a subset of POTS patients, confirming that structural nerve abnormalities may be present in some cases.
Chronic Inflammation
Inflammation affects blood vessels, nervous system signaling, circulation, and mitochondrial energy production.
Chronic inflammatory activation may contribute to:
fatigue
brain fog
exercise intolerance
nervous system hypersensitivity
worsening autonomic instability
This is one reason many POTS patients also experience overlapping inflammatory or immune-related conditions.
MCAS, Connective Tissue Disorders & the POTS Triad
These three conditions — POTS, Mast Cell Activation Syndrome (MCAS), and hypermobile Ehlers-Danlos Syndrome (hEDS) — co-occur so frequently that researchers and clinicians have begun referring to them informally as "the trifecta.”
In hypermobile EDS and related connective tissue disorders, laxity in blood vessel walls allows excessive venous pooling upon standing — directly worsening orthostatic intolerance. The same connective tissue abnormalities that cause joint hypermobility affect every blood vessel in the body.
MCAS adds another layer — mast cells release histamine and other inflammatory mediators that cause widespread vasodilation, further reducing blood flow to the brain upon standing. Studies suggest up to 50% of POTS patients meet criteria for MCAS, and a significant proportion also have hEDS or hypermobility spectrum disorder.
When all three are present, treating POTS without addressing the others is like bailing water from a leaking boat. Our evaluation screens for all three — and our care plan addresses each one.
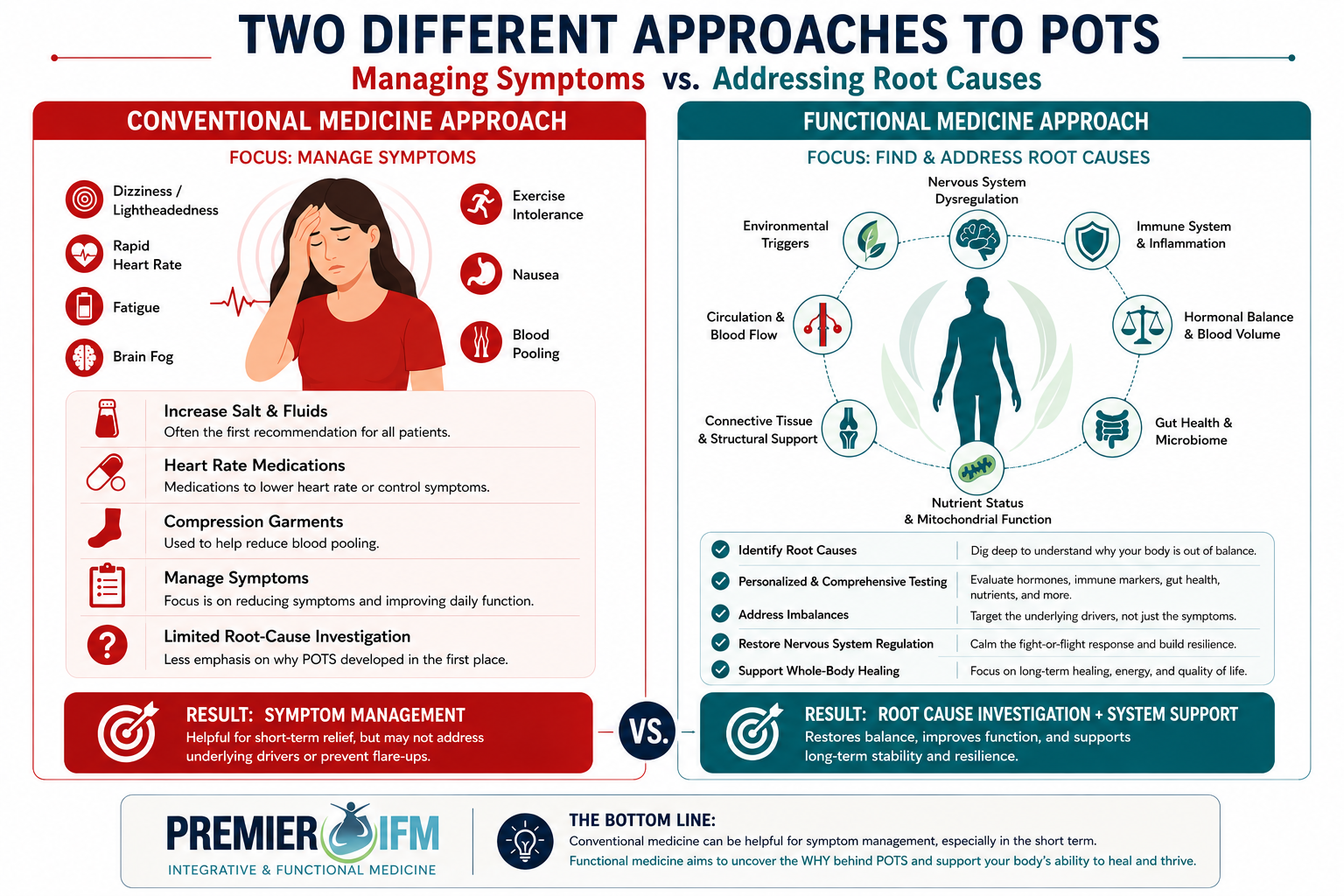
Conventional vs. Functional Medicine for POTS
Conventional POTS management typically focuses on symptomatic relief — beta blockers to slow heart rate, fludrocortisone to increase blood volume, midodrine to constrict blood vessels, compression garments, and increased salt and fluid intake. For some patients these provide meaningful relief. For many, they do not — because the underlying drivers are never addressed.
Functional medicine does not replace these interventions when they are appropriate. What it adds is a systematic investigation into why the autonomic nervous system became dysregulated — and a targeted plan to correct those upstream imbalances.
What our functional medicine evaluation for POTS includes:
Advanced autonomic and cardiovascular markers beyond standard labs
Autoimmune antibody panels including adrenergic receptor autoantibodies
Comprehensive hormonal evaluation — aldosterone, renin, cortisol, catecholamines
Gut health assessment — microbiome, intestinal permeability, SIBO testing
Mast cell activation markers — tryptase, histamine, prostaglandins
Nutritional deficiency screening — B12, thiamine, iron, vitamin D, magnesium
Inflammatory and neuroinflammatory markers
Chronic infection screening — EBV, Lyme, mycotoxins, COVID antibody patterns
Connective tissue and hypermobility assessment
Review of all prior testing, diagnoses, and interventions
Research note on infrared sauna and POTS: A study published in the Japanese Circulation Journal found that regular far-infrared sauna sessions over 15 days significantly improved symptoms of chronic heart failure patients with orthostatic intolerance — including improvements in heart rate variability, plasma volume, and exercise tolerance. This "thermal therapy" approach is now being studied more broadly for dysautonomia.
If you have been told your labs are normal but you still feel this way — let's look deeper.
Your Questions, Answered
-
POTS can have many different underlying causes and contributing factors. Common drivers include nervous system dysregulation, viral illness, autoimmune activity, chronic inflammation, hormonal imbalances, low blood volume, connective tissue disorders, and gut dysfunction.
For many patients, POTS develops after a significant stressor such as:
COVID-19 or another viral infection
Surgery
Pregnancy
Physical trauma
Chronic stress
Functional medicine focuses on identifying the underlying factors contributing to symptoms rather than only managing heart rate.
-
In POTS, the autonomic nervous system has difficulty regulating circulation when you stand upright.
Blood can pool in the lower body instead of returning efficiently to the heart and brain. As a result, the heart beats faster to compensate, which may cause:
dizziness
rapid heart rate
fatigue
lightheadedness
brain fog
This is known as orthostatic intolerance.
-
Yes. POTS is considered a disorder of the autonomic nervous system—the system responsible for controlling automatic body functions such as, heart rate, blood pressure, digestion, temperature regulation, and circulation.
Many POTS symptoms occur because the nervous system struggles to properly regulate these functions when the body changes position.
-
Research suggests that POTS may have an autoimmune component in some patients.
Studies have identified autoantibodies that may interfere with receptors involved in autonomic nervous system regulation. Many patients also report symptom onset after viral illness or immune activation.
While not every case is autoimmune, immune dysregulation appears to play an important role in a significant subset of POTS patients.
-
Yes. Chronic inflammation can worsen POTS symptoms by affecting the nervous system, circulation, blood vessels, and the body’s ability to regulate stress and energy production. Many patients notice increased fatigue, brain fog, dizziness, and exercise intolerance during periods of higher inflammation. This is one reason POTS commonly overlaps with post-viral illness, autoimmune conditions, and other inflammatory disorders. Functional medicine focuses on identifying and reducing underlying sources of inflammation to help improve autonomic stability and overall quality of life.
-
Yes. Functional medicine helps by identifying and addressing the root causes contributing to POTS in order to improve symptoms and overall function.
Rather than focusing only on heart rate, functional medicine looks at underlying factors such as:
nervous system dysregulation
inflammation
immune dysfunction
gut health
hormone imbalances
nutrient deficiencies
By supporting the body as a whole, many patients experience improvements in dizziness, fatigue, brain fog, circulation, and quality of life.
-
Yes. Many POTS patients experience digestive symptoms such as bloating, nausea, reflux, constipation, IBS, or SIBO.
The gut and nervous system are closely connected through the gut-brain axis and enteric nervous system. Gut inflammation, microbiome imbalances, and immune activation may contribute to autonomic dysfunction in some patients.
-
POTS is a physiological condition—not simply anxiety.
However, POTS symptoms can sometimes mimic anxiety because both conditions involve activation of the nervous system and adrenaline pathways.
Rapid heart rate, dizziness, shakiness, and sweating are common in both conditions, which is why many POTS patients are initially misdiagnosed. While stress can worsen symptoms, POTS is a real autonomic nervous system disorder.
-
Yes. Long COVID is now recognized as a major trigger for POTS (Postural Orthostatic Tachycardia Syndrome) and autonomic nervous system dysfunction.
Many patients develop symptoms such as dizziness, rapid heart rate, fatigue, brain fog, exercise intolerance, and palpitations after recovering from COVID-19. Research suggests that inflammation, immune dysregulation, nervous system dysfunction, and vascular changes caused by the virus may contribute to the development of POTS in some individuals.
For many people, symptoms begin weeks or even months after the initial infection and can significantly impact daily function and quality of life.
-
POTS (Postural Orthostatic Tachycardia Syndrome) is typically diagnosed using a combination of symptom history, physical examination, and heart rate measurements during changes in posture.
One of the primary diagnostic criteria is an increase in heart rate of 30 beats per minute or more within 10 minutes of standing (without a significant drop in blood pressure). In adolescents, the increase is typically 40 beats per minute or more.
Common tests used to evaluate POTS include:
Tilt table testing
Active stand testing
Heart rate and blood pressure monitoring
Blood work to rule out other conditions
Because POTS symptoms often overlap with anxiety, chronic fatigue, and other disorders, many patients go years without a proper diagnosis. A thorough evaluation is important to identify both autonomic dysfunction and any underlying contributing factors.
-
recovery varies from person to person.
Research shows that many adolescents and young adults experience meaningful symptom improvement over time. A 2016 Journal of Pediatrics study found that approximately 86% of adolescents with POTS reported improvement within about 5 years, with some experiencing complete symptom resolution.
Children’s National Hospital also reports that many pediatric patients improve substantially, although recovery may take months or even several years.
For adults, the course of POTS is often more variable. Johns Hopkins Medicine notes that some patients recover fully, while others experience symptoms that fluctuate or “flare” over time.
What’s important is that POTS is not necessarily a permanent or progressively worsening condition.
Research increasingly suggests that outcomes are strongly influenced by whether underlying contributing factors are identified and addressed. These may include:
post-viral inflammation
autoimmune activity
nervous system dysregulation
nutrient deficiencies
gut dysfunction
hormonal imbalances
Patients who address the root causes contributing to autonomic dysfunction often experience meaningful improvements in symptoms, energy, function, and quality of life.
For many people, POTS does not have to be a life sentence—and improvement is absolutely possible with the right support and treatment approach.
More Light reading. Check out our related Blog posts